We are proud that BalanceBelt is collaborating on a clinical study with leading experts in the field of vestibular disorders at Johns Hopkins University. This research brings together the expertise of Michael Schubert and Kathleen Cullen, supported by Michela De Marzi.

Professor of Otolaryngology-Head and Neck Surgery

Master’s student in Biomedical Engineering

Professor of Biomedical Engineering
Together, this multidisciplinary team of clinicians and scientists is advancing our understanding of balance disorders and exploring how innovative solutions like BalanceBelt can improve patient outcomes in real-world settings. Their work bridges clinical practice, neuroscience, and engineering, combining deep scientific insight with a strong focus on practical impact for patients living with severe vestibular dysfunction.
This collaboration marks an important step in generating robust clinical evidence, while further exploring how wearable haptic technology can support balance, mobility, and independence in daily life.
Background & expertise
Could you briefly describe your professional journey and what led you to specialize in Physical Medicine & Rehabilitation and Otolaryngology?
We are a team of clinicians and scientists with a deep interest in improving the lives of individuals living with vestibular disorders. Our work has been shaped by a shared recognition that balance dysfunction is both highly debilitating and often under-addressed. This motivated us to pursue careers that bridge clinical care and research, with the goal of developing more effective diagnostic tools and rehabilitation strategies.
What is your current role at Johns Hopkins University, and what are your main clinical and research interests?
Michael: My lab examines the oculomotor and gait strategies recruited by the brain to compensate for the impairments associated with vestibular disorders. We focus on understanding how patients adapt their movement patterns and how these adaptations can be enhanced through targeted rehabilitation.
Kathleen: My research focuses on how the brain encodes and integrates vestibular signals during natural behaviors, including gaze control and locomotion. We study the neural mechanisms underlying balance and self-motion perception, with a particular emphasis on the objective quantification of how these processes are altered following vestibular loss and how they can be restored or compensated for through intervention.
Connection to BalanceBelt
When and how did you first come across BalanceBelt, and what sparked your interest in the technology?
We first learned about the BalanceBelt through professional meetings and the work of Herman Kingma. What immediately stood out was its elegant approach to sensory substitution—providing continuous, intuitive feedback about body orientation in space.

From a clinical perspective, what problem does BalanceBelt aim to solve for your patients?
We are investigating how the BalanceBelt can lead to objective improvements in patients with bilateral vestibular hypofunction. These individuals lack a critical sensory system for balance, and the device offers a potential way to augment their perception of orientation and movement in everyday life.
Clinical study
Could you describe the scope and design of the upcoming clinical study with BalanceBelt?
We are planning a longitudinal study in which patients with bilateral vestibular hypofunction will take the BalanceBelt home and wear it during daily activities over an extended period. We will assess both clinical outcomes and detailed kinematic measures at multiple time points to evaluate adaptation and functional improvement.
What makes this study novel compared to previous research in balance disorders or sensory substitution?
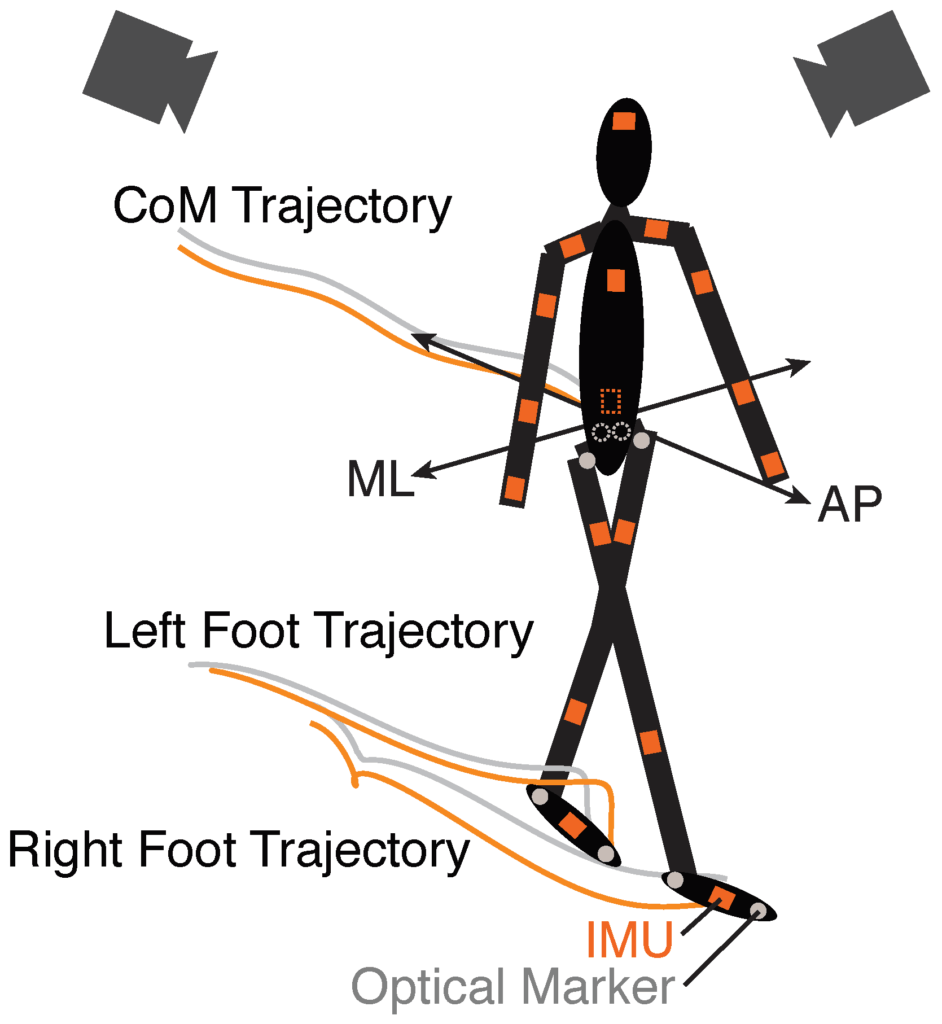
Our study combines real-world use of a sensory substitution device with advanced quantitative analysis of gait and posture using wearable IMUs. This allows us to move beyond traditional clinical scales and directly measure how movement strategies evolve over time.
Which patient population are you focusing on, and why?
We are focusing on individuals with bilateral vestibular loss, as they experience profound balance deficits and have limited treatment options. This population stands to benefit most from technologies that can substitute or augment missing sensory information.
What key outcomes or metrics will you be looking at to determine effectiveness?
IMU based metrics that distinguish fall risk behavior from healthy controls.
We will focus on IMU-based kinematic metrics that capture features of gait stability and variability known to be associated with fall risk. These objective measures will be compared to healthy controls and tracked longitudinally to assess improvement.
Scientific & clinical impact
How do you see haptic feedback contributing to balance rehabilitation?
Haptic feedback provides an additional sensory channel that the brain can learn to integrate with existing visual and proprioceptive inputs. While the precise mechanisms remain to be fully understood, it offers a promising way to enhance spatial awareness and stability, particularly in patients who lack vestibular input.
If successful, how could this technology change current standards of care for patients with balance disorders?
If effective, this technology could become an important adjunct to rehabilitation, offering patients a continuous source of feedback during daily activities. This could accelerate adaptation, improve functional mobility, and ultimately reduce fall risk.
What are the biggest challenges in translating technologies like this into routine clinical practice?
One major challenge is clinical adoption. There is still limited awareness—both among clinicians and patients—that balance can be trained and improved. Integrating new technologies into standard care pathways will require education, validation, and demonstration of clear functional benefits.
Collaboration
Could you describe the value of a multidisciplinary approach in this project, like the collaboration with Kathleen Cullen’s group?
The combination of clinical insight and the Cullen group’s engineering expertise allows us to move efficiently from concept to implementation. This collaboration ensures that the questions we ask are clinically meaningful while the methods we use are technically rigorous.

How does combining expertise from ENT, rehabilitation, and engineering strengthen the study?
By integrating perspectives from ENT, rehabilitation, and engineering, we can address the problem at multiple levels—from underlying neural mechanisms to real-world patient function. This multidisciplinary approach enables more comprehensive solutions than would be possible within a single field.